🍁Greetings to one and all going through my E log!!
🩺This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment.
I am Nomika. Alli (Roll no 179) of 8th Sem MBBS.
A 44 yr old man , daily wage laborer R/O Miryalaguda came to the OPD on 5th September 2023 with chief complaints of abdominal pain , vomitings and constipation and fever at nights since 5 days.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 18 days back and then developed pain in the epigastric region and left hypochondriac region followed by high grade fever(at nights only = nocturnal), intermittent a/o chills , one episode of vomiting daily morning contained food particles, bilious, non projectile, non blood tinged, odorless. 4 days later, He got admitted in a local hospital and was diagnosed as ACUTE PANCREATITIS . and was discharged 2days later. Patient was advised to take few medications and Symptoms have completely disappeared in 4 days. Again After 4 days the patient developed pain abdomen similar to the previous episodes, stabbing type near epigastric region and left hypochondriac region, insidious onset, intermittent, gradually progressive , radiating to back. Pain aggravated on coughing. Similar episodes of vomitings occurred (one episode daily, contained food particles, bilious, non projectile, non blood tinged, odorless) and had night raise in temperature (nocturnal fever) a/o chills, intermittent, high grade and also had generalized body pains. He had c/o constipation since 5 days. Flatus passed.
No H/O loose stools, giddiness, polyuria, bleeding, dehydration, weight loss, oily stool, poor appetite, itchy skin, dark urine
No H/O chest pain, palpitations, SOB, Orthopnea, PND
H/o Alcohol binge drinking since 25 years (one quarter = 180ml daily)
Last consumption August 21st 2023
He wakes up at 6am ,has his breakfast by 7:30am and goes to work ,has his lunch by 1:30pm, takes alcohol (90 ml) ,returns home by around 6pm ,takes alcohol (90ml) ,has his dinner by around 9pm and goes to bed by 9:30pm.
Story from April 2023:
This 44 yr old man who is a known binge alcoholic since 25 yrs had c/o pain abdomen (in epigastric area, stabbing type , gradually progressive, radiating to back) for a week, generalized body weakness, night fever a/o chills and vomitings. He went to a local hospital where he was admitted for a week and given medications. At discharge, he was advised to stop alcohol consumption and take few medication (followed).
After two months of abstinence, i.e; from june 2023, he started consuming alcohol (180 ml daily) again (no symptoms).
Three months passed away without any symptoms (on alcohol).
From August 18th 2023, he started developing pain abdomen in epigastric region and left hypochondriac area, stabbing type, gradually progressive, insidious, intermittent, radiating to back. He had raised temperature at nights a/o chills (high grade). He had one episode of vomiting everyday in the morning ( contained food particles, bilious, non projectile, non blood tinged, odorless) . He also have c/o generalized body pains and constipation.
On August 22nd ,2023 he went to a local hospital and diagnosed with Acute Pancreatitis and Left minimal pleural effusion was admitted in hospital for 2 days and discharged. He was given a course of medications to be followed until 26th august. After completing the course, all his symptoms are resolved and he was asymptomatic for the next 4 days.
On September 1st, he got his pain abdomen back , constipation (flatus passed), vomiting (one episode daily) a/o fever and generalized weakness. He waited for 5 days thinking the symptoms would resolve and got admitted in KIMS, Narketpally on 5th September.
PAST HISTORY:
N/K/C/O DM, HTN, TB, Asthma, CAD, CVD, Epilepsy,..
H/O similar complaints in the past.
SURGICAL HISTORY:
not significant
FAMILY HISTORY: Not significant
PERSONAL HISTORY:
Married
Daily wage laborer
Diet: mixed
Appetite: normal
bladder movements: regular
Sleep: adequate, not disturbed
Addictions: binge alcoholic since 25 yrs (180ml= one quarter daily)
Last consumed 15days back
Allergies: no known
PHYSICAL EXAMINATION:
GENERAL:
Patient is conscious , coherent and cooperative to time place and person.
Ht: 160cm Wt: 60kg
Pallor: present
Icterus: no
Clubbing: no
Cyanosis: no
Lymphadenopathy: no
Edema: no
Vitals: BP: 110/70mmHg
Temp: 99.8F
PR: 115 bpm
RR: 15 cpm
SpO2: 99%
GRBS: 94 mg%
SYSTEMIC EXAMINATION:
CVS: S1 S2 heard
no thrills
no murmurs
RS: no dyspnoea
no wheeze
central position of trachea
normal vesicular breath sounds +
ABDOMEN:
Inspection: scaphoid shape
umbilicus central and inverted
no scars, sinuses, engorged veins
no visible gastric peristalsis
no visible mass
All quadrants of abdomen are moving accordingly with respiration.
Palpation: febrile 99.8F
Tenderness present
Left iliac fossa
guarding present
no rigidity
no organomegaly
bowel sounds: sluggish
no fissures
no palpable mas
normal hernial orifices
liver not palpable
CNS: conscious
coherent speech
no neck stiffness
kernig's sign negative
cranial nerves, motor system , sensory system: intact, normal
Glasgow scale: E4V5M6 =15
PHYSICAL EXAMINATION:
INVESTIGATIONS:
5-9-23
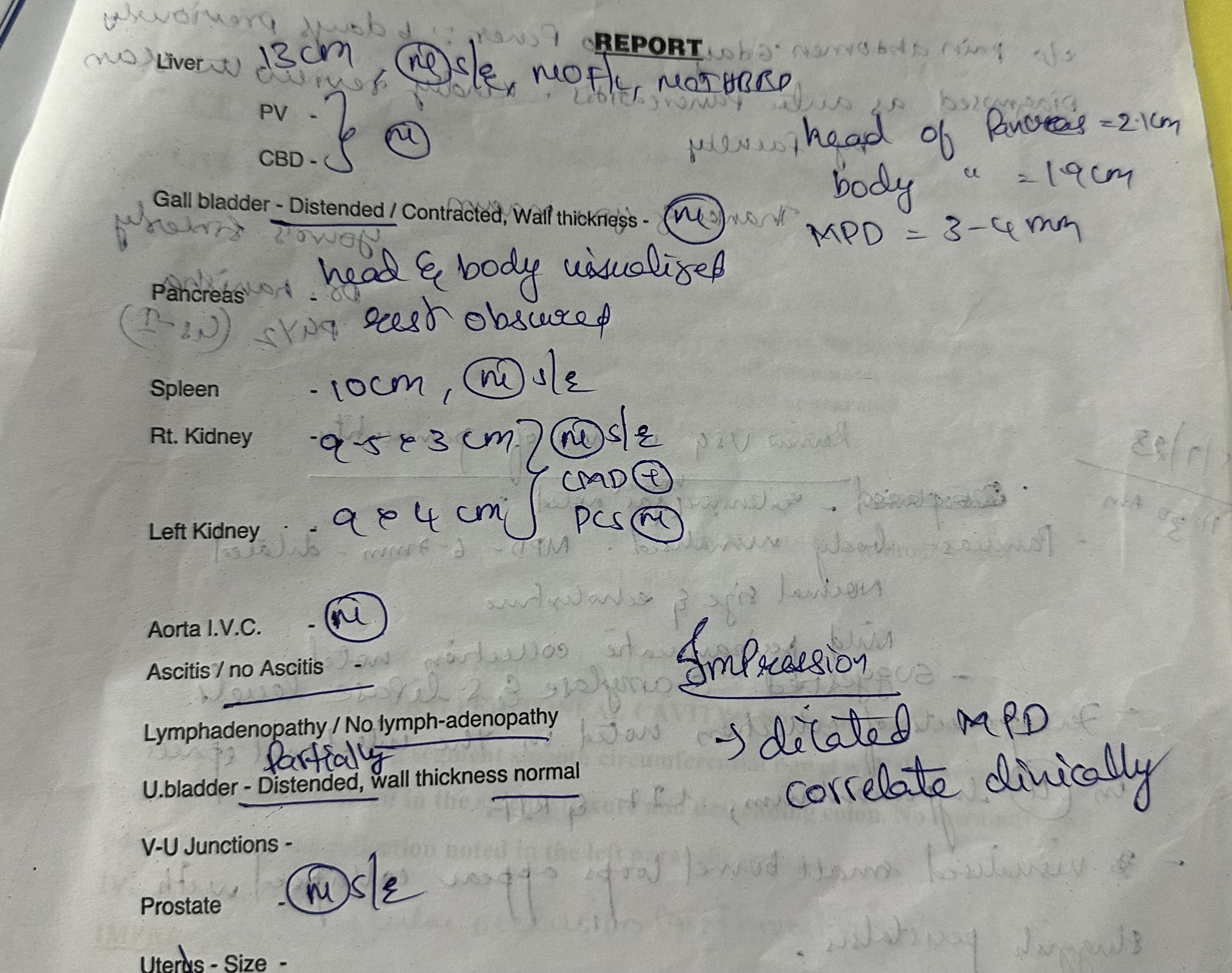
USG
6-9-23
PROVISISONAL DIAGNOSIS:
ACUTE ON CHRONIC PANCREATITIS
Binge Alcohol drinker since 25 yrs



























































.png)
.png)

