🍁Greetings to one and all going through my E log!!
🩺This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment.
I am Nomika. Alli (Roll no 179) of 8th Sem MBBS.
A 58 year old female, house-wife by occupation R/O Yadagiri gutta came to the OPD on 29th August 2023 with chief complaints of :
both right upper limb and lower limb weakness since one day
unable to talk (loss of speech) since 4-5 hours
mouth deviated to left side since 4 hours
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic one day ago then she developed weakness in both upper and lower limbs of right side but was able to feel senses of both limbs and eat with right upper limb. After 20hrs (one day approx.) patient was unable to speak i.e; sudden loss of speech and her mouth deviated to left side.
No H/O involuntary movements
No H/O Loss of consciousness
No H/O loss of sensation
No H/O up rolling of eyes
No H/O involuntary passage of urine and feces
No H/O tremors
No H/O fever
No H/O trauma to head
No H/O sleep disturbances
Her daily routine is waking up at 6: 30 am, drinks plain milk(without sugar) at 7:00 am, breakfast (4 idlies with karam podi daily ) at 8:00 am. She used to have her lunch as rice and curry (less spicy and less /no salt) at 1: 00 pm and some milk(without sugar) at 5 :00 pm . She usually haves her dinner as rice with curry (less spicy and less /no salt) at 9:00pm and goes to bed by 9:30 pm.
The patient used to walk only with support from past 2 years but used to speak normally before this episode of loss of speech 5 hours ago.
PAST HISTORY:
K/C/O HTN since May 2021. On unknown medication (2.5???)
K/C/O CVA- Right hemiparesis since 2 yrs. course completed (unknown medication)
Story in May 2021:
While this absolutely normal female is travelling on a two wheeler for 15km and when her destination has arrived , she was not able to get down the vehicle and felt tingling sensation with numbness in her right upper and lower limb. She was taken home and those symptoms didn't subside even after 6 hours, didn't perceive sensations, able to talk normally, no mouth deviation, no involuntary movements, no up rolling of lids, no incontinence of urine or feces, no loss of consciousness, no trauma to head, no tremors . She was rushed to a local hospital where she was diagnosed PARALYSIS and asked them to go to a higher hospital. She was admitted for 15 days in hospital and given medications. MRI/ CT?? was taken which was interpret to family as bleeding hemorrhage in brain?? While Discharge they were told that the size of hemorrhage has decreased and bleeding stopped and asked to follow up a course of drugs ( MVT & ?? & ??) and advised to go for physiotherapy for 2-3 months.(taken)
She was also diagnosed with Hypertension and given medications which she is still continuing now.
N/K/O DM, CAD, TB, Epilepsy, Asthma, Thyroid,..
SURGICAL HISTORY:
Patella surgery 7 yrs ago
LSCS 28yrs ago
FAMILY HISTORY:
Not significant
PERSONAL HISTORY:
Married
House- wife
Diet: mixed (less spicy, less salt, less oil, no sugar, drinks only hot water)
Appetite: normal
Bowel & bladder movements: regular
Sleep: adequate, not disturbed
Addictions: none
Allergies: no known
MENSTRUAL HISTORY: Menopause 10yrs ago
OBSTETRIC HISTORY: G5P4L5
First preg.: FTNVD Male alive and healthy
Second preg.: FTNVD Twin females alive and healthy
Third preg.: FTNVD Female alive and healthy
Fourth preg.: FTLSCS Male alive and healthy
PHYSICAL EXAMINATION:
GENERAL:
Patient is conscious , not coherent and cooperative to time place and person.
Ht: 155cm Wt: 50kg
Pallor: no
Icterus: no
Clubbing: no
Cyanosis: no
Lymphadenopathy: no
Edema: no
Vitals: BP: 110/80mmHg
Temp: Afebrile
PR: 102 bpm
RR: 24 cpm
SpO2: 98%
GRBS: 170 mg%
SYSTEMIC EXAMINATION:
CVS: S1 S2 heard
no thrills
no murmurs
RS: no dyspnoea
no wheeze
central position of trachea
normal vesicular breath sounds +
ABDOMEN: Shape: scaphoid
no tenderness
normal hernial orifices
no free fluid
no bruits
liver and spleen not palpable
CNS: altered sensorium
incoherent speech
no neck stiffness
kernig's sign negative
cranial nerves, motor system , sensory system: intact, normal
Glasgow scale: E4V1M6

Cerebellar signs- unable to elicit





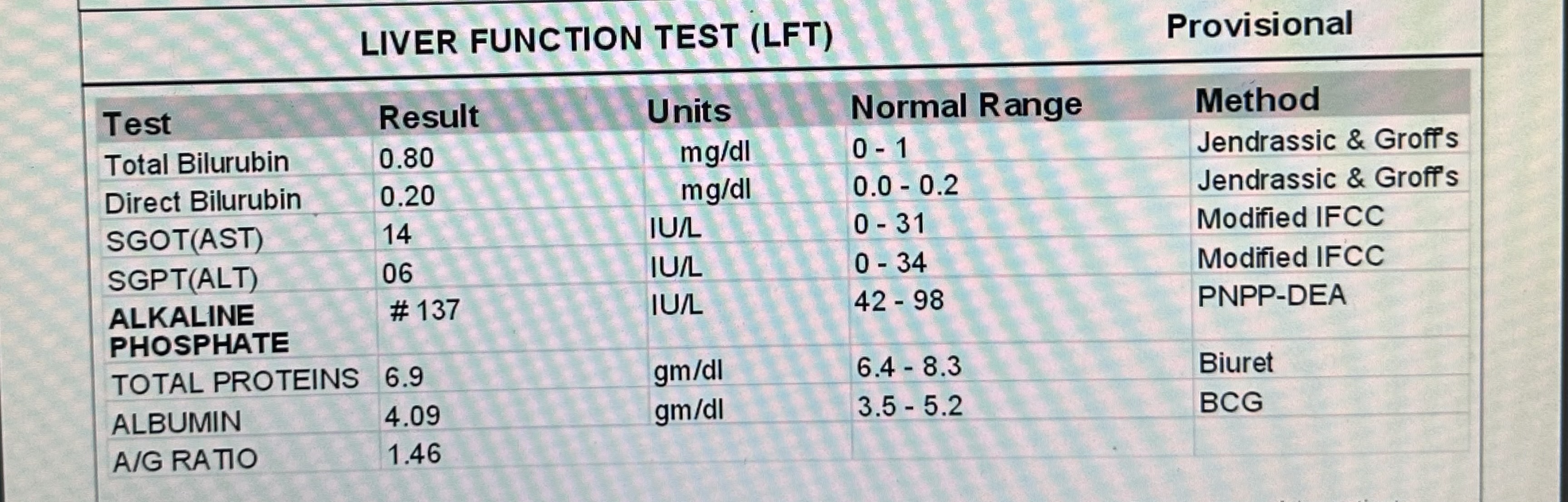
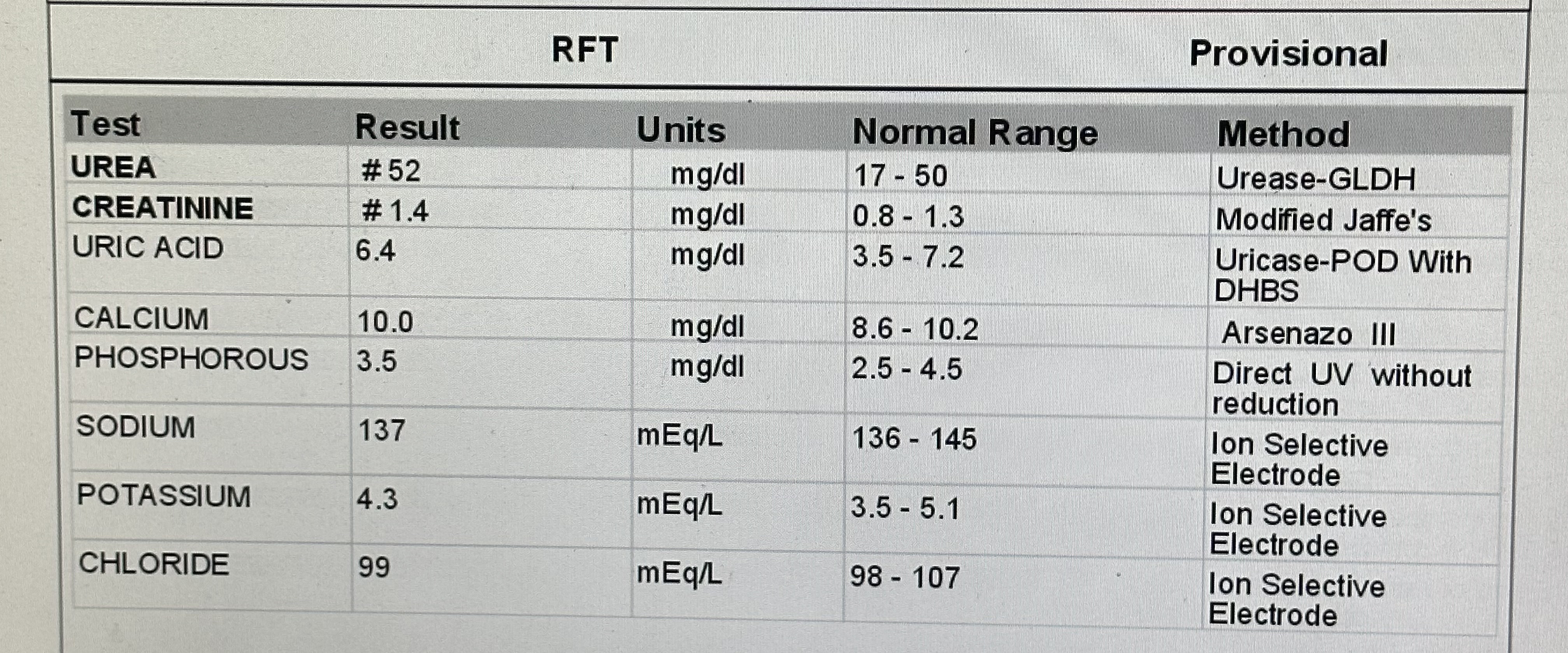
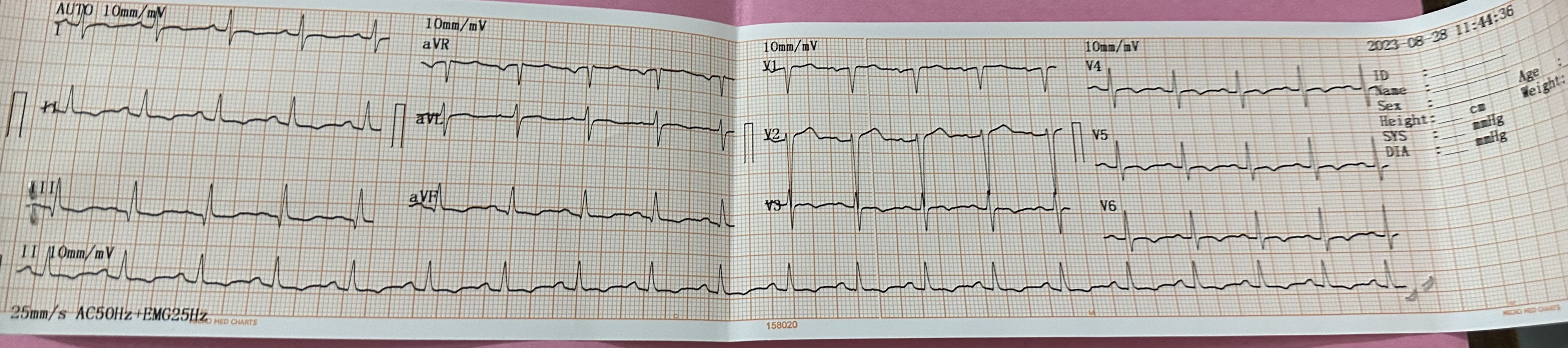
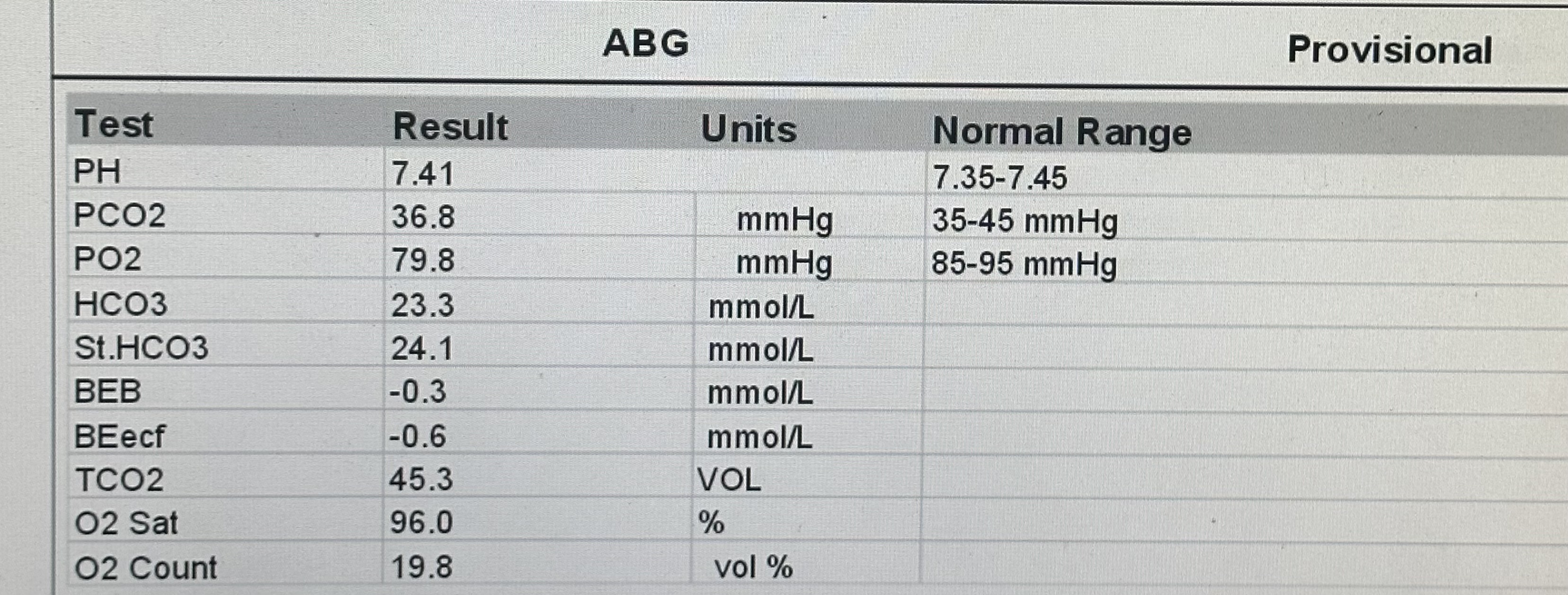
INVESTIGATIONS:
29-8-23













RECURRENT CVA
with HEMORRHAGIC INFARCT in parieto-occipital region
with K/C/O HTN since 2 yrs
BROCA'S APHASIA??
















































.png)
.png)

