🍁Greetings to one and all going through my E log!!
🩺This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment.
I am Nomika. Alli (Roll no 179) of 8th Sem MBBS.
A 69 year old male Resident of Mellacheruvu (Suryapet) , shopkeeper by occupation came to the OPD on 24th August 2023 with complaints of 10-12 episodes of greyish black colored vomitings since one day.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic one days back and then developed mild epigastric pain and discomfort in the chest on the morning of 23rd August 2023. After lunch he developed 10-12 episodes of non projectile vomiting which is watery, containing food particles, greyish black (bilious ?) in color , non foul smelling, non blood tinged , continuing throughout that day and night and morning of 24th August 2023.
No H/O abdominal pain , loose stools, giddiness
Patient was irritable that night(23rd august 2023) and didn't sleep .
No H/O Fever, cough
His daily routine is waking up at 6: 00 am, drinks tea at 7:00 am, breakfast (idli/ dosa/ other South Indian breakfast) at 8:00 am and go to work. He used to have his lunch as rice and curry at 1: 00 pm and some tea with biscuit at 5 :00 pm .He usually haves his dinner as chapati/rice with curry/ other breakfast at 9:00pm and goes to bed by 10:00 pm.
The patient used to lead a normal life until one day before these episodes.
HISTORY OF PAST ILLNESS:
K/C/O DM type II since 20 years.
On Biphasic insulin: 100(before breakfast)------x------150(before dinner)
N/K/C/O: HTN/ TB/ asthma/ CAD/CVD/ Epilepsy
No similar complaints in the past
No previous reflux disorders
SURGICAL HISTORY: none
FAMILY HISTORY: Patient's father is known Diabetic.
N/K/C/O: HTN/ TB/ asthma/ CAD/CVD/ Epilepsy
PERSONAL HISTORY:
Married
Shop keeper by occupation
Diet: Vegetarian
Appetite: Normal
Sleep: adequate
Bowel and bladder movements: Regular
Addictions: none
Allergies: no known
GENERAL EXAMINATION:
Patient is conscious, coherent, cooperative to time, place, person.
Ht: 165cm wt: 75kg
Pallor: no
Icterus: no
Cyanosis: no
Clubbing: no
Lymphadenopathy: no
Edema: no
Malnutrition: no
Dehydration: no
Vitals: BP: 160/90 mmHg
PR: 102bpm
RR: 18 cpm
Temp: 98.4°F
SpO2: 98%
GRBS: 335mg%
SYSTEMIC EXAMINATION:
CVS: S1 S2 heard
no thrills
no murmurs
RS: no dyspnoea
no wheeze
central position of trachea
normal vesicular breath sounds +
ABDOMEN: Shape: scaphoid
no tenderness
normal hernial orifices
no free fluid
no bruits
liver and spleen not palpable
CNS: conscious
normal speech
no neck stiffness
kernig's sign negative
cranial nerves, motor system , sensory system: intact, normal
Glasgow scale: E4V5M6
Cerebellar signs- no
finger nose in coordination: yes
Knee heel in coordination: yes
GAIT: normal
MUSCULOSKELETAL SYSTEM: normal
PROVISIONAL DIAGNOSIS:
DIABETIC KETOSIS
with TYPE II DM
with ??DENOVO HTN
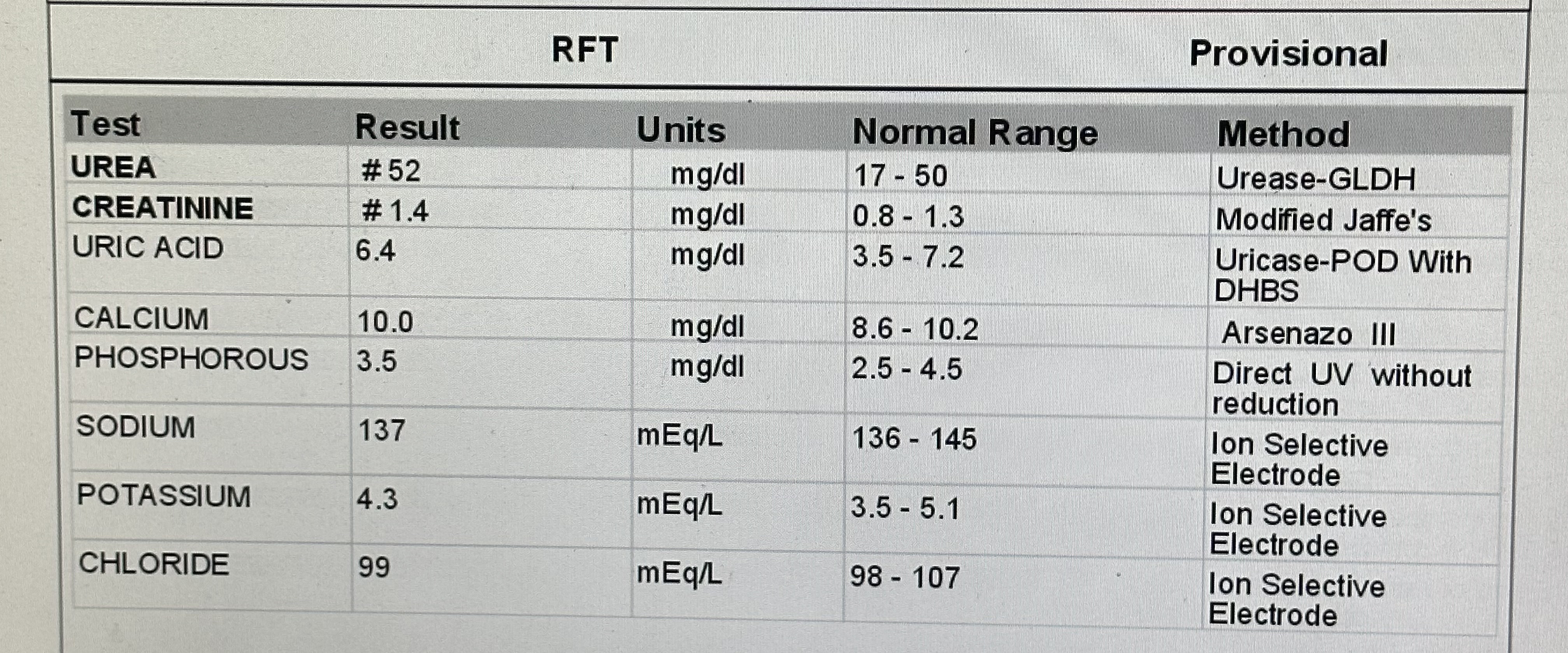
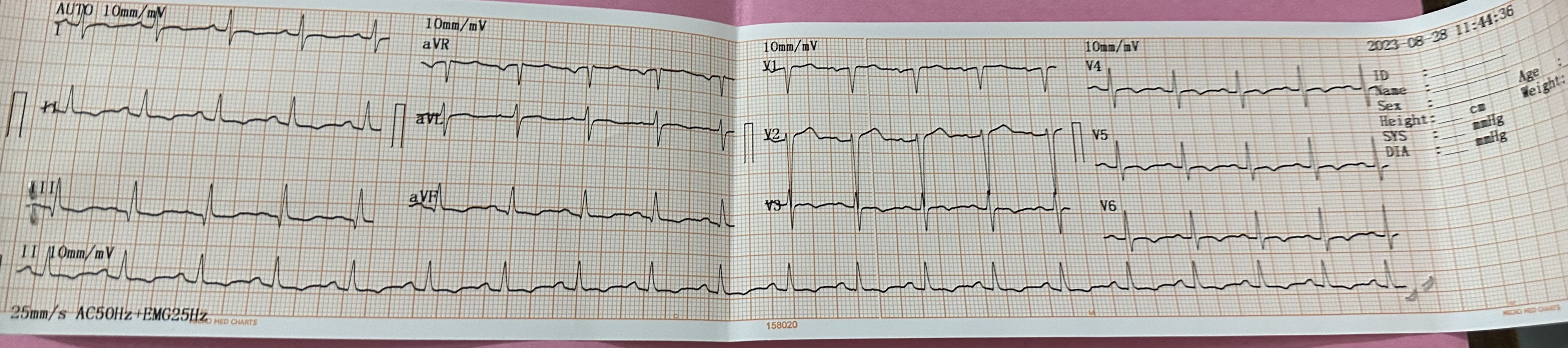
PHYSICAL EXAMINATION:

























.png)
.png)


No comments:
Post a Comment