🍁Greetings to one and all going through my E log!!
🩺This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment.
I am Nomika Alli (Roll no 179) of 8th Sem MBBS.
A 65 year old Male, R/O Nalgonda, came to the OPD on 13th August 2023 with complaints of Fever since 6 days and lower limb swelling and pain since 2 days
HISTORY OF PRESENT ILLNESS:
Patient has developed fever associated with chills one week back , continuous , relieved on taking paracetamol. After 4 days of onset of fever, patient developed swelling of left lower limb which initially started at level of foot and then gradually progressed to below knee joint which is a/o pricking type of pain.
No aggravating and relieving factors.
Associated with discharge at left greater toe i.e; seropurulent in nature
H/O draining wound/ sinus (watery / pus ??) with mild edema from last 20 yrs near left ankle after an injury to left ankle/ toe?? 20 yrs back. Dressing is done few times in this span of 20 yrs
No H/O pale limbs , SOB, rash, lightheadedness
No H/O vomiting, loss of appetite, burning micturition.
His daily routine is waking up at 6: 00 am, drinks tea at 7:00 am, breakfast as rice and curry at 8:00 am . He used to have his lunch as rice and curry at 1: 00 pm .He usually haves his dinner as rice and curry at 8:00pm and goes to bed by 9:00 pm.
The patient used to lead a normal life before this episode of fever and used to walk normally and freely.
HISTORY OF PAST ILLNESS:
N/K/C/O DM, HTN, Asthma, CAD, CVD, Thyroid, epilepsy
H/O TB (Pulmonary koch's) 8 yrs ago for which treatment was taken. (ATT drugs)
H/O ulcer at left ankle 20yrs ago
Patient is Deaf since childhood. (cong / acquired???)
SURGICAL HISTORY: H/o cataract surgery for rt eye
FAMILY HISTORY:
N/K/C/O DM, HTN, Asthma, Epilepsy, CAD, CVD
This patient's elder brothers died with lower limb related disorders/ pathologies?? few years back.
His younger brother passed away with stomach TB when he was 25 yrs .
PERSONAL HISTORY:
Married
Daily wage laborer by occupation. stopped working few yrs ago.
Diet: Mixed
Appetite: Normal
Sleep: adequate
Bowel and bladder movements: Regular
Addictions: Alcohol occasionally
Allergies: no known
GENERAL EXAMINATION:
Patient is conscious, coherent, cooperative to time , place, person.
Ht: 155cm Wt: 58 kg
Pallor: present
Icterus: absent
Clubbing: absent
Cyanosis: absent
Koilonychia: absent
Lymphadenopathy: absent
Edema: left lower limb cellulitis
right LL edema
Vitals: Temp: 99.4F
BP: 70/40 mmHg
PR: 121 bpm
RR: 21 cpm
SpO2: 90%
GRBS: 63 mg%
SYSTEMIC EXAMINATION:
Limb examination (L/E)-
- Left lower limb edema upto knee joint
- local raise of temperature
- tenderness present
- edema: pitting type
- peripheral pulses not felt due to edema
CVS:
S1 S2 heard
No murmurs
No thrills
RS:
Crepts +
Lt. IAA
No dyspnoea
No wheeze
Central position of trachea
NVBS +
ABDOMEN:
Shape of abdomen: scaphoid
No tenderness
No palpable mass
Hernial orifices: Right inguinal hernia present
No bruits
Liver and spleen- not palpable
Bowel sounds heard
CNS:
Conscious
no neck stiffness
kernig's sign negative
cranial nerves: normal
motor - intact
sensory - intact
Glasgow scale E4V3M6 = 13/15
Cerebellar signs- no
Finger nose in coordination: yes
knee heel in coordination: yes
LIMB SCORE:
Left LL: -1/5 (Left LL monoplegia)
Right LL: -4/5
Upper limbs: -2/5
Paraplegia?? Hemiplegia?/ Quadriparesis??
Knee hammer :rt knee reflex: elicited sometimes
ankle reflex: edema and pain+
left knee: pain
MUSCULOSKELETAL SYSTEM: normal
SKIN: normal
ENT: normal
TOOTH & ORAL CAVITY: normal
PHYSICAL EXAMINATION:
Dressed lower limb with MgSO4
Rt. knee: resembling leathery appearance on touching
indurated
peau d orange???
2° vitiligo
Left LL:
Left knee: smooth to touch
Pallor present
edema of both wrists and hands due to thrombus
INVESTIGATIONS:
Investigations done on 12th august 2023(local hospital)
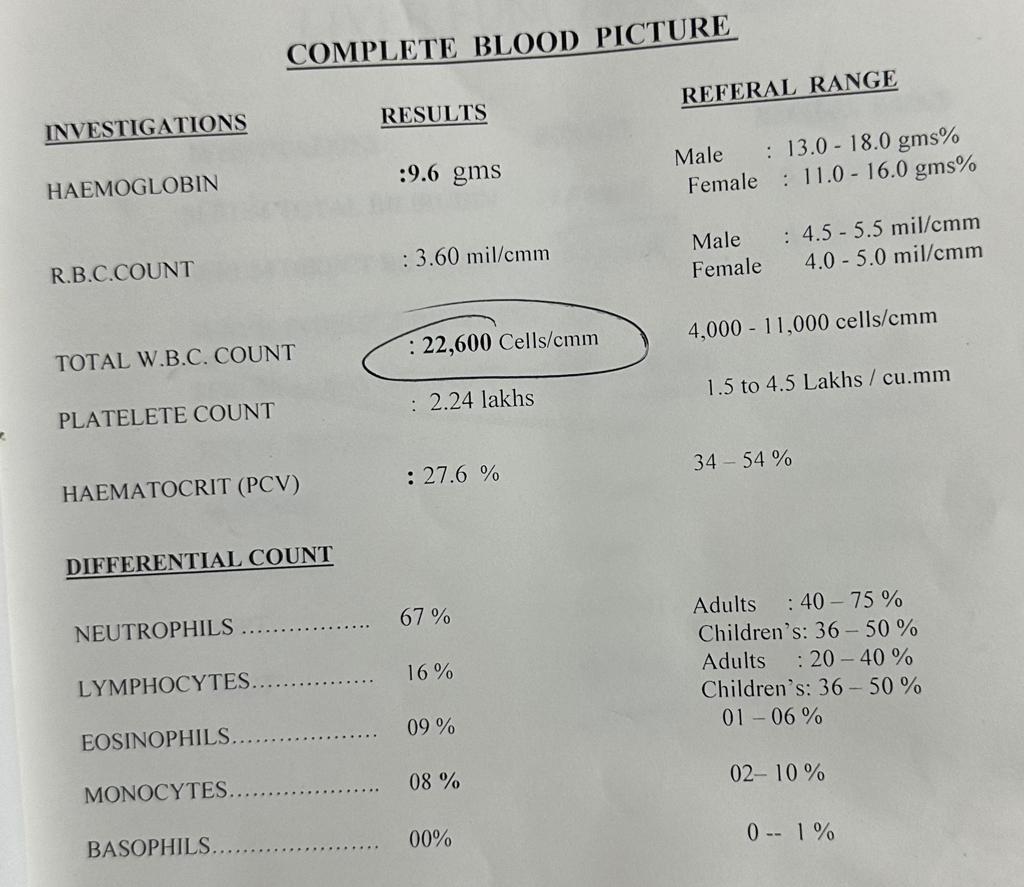
CBP: Increased total WBC count
decreased Hb
LFT: increased BR
increased S. AKP
increased SGOT
RFT: increased S. creatinine
increased uric acid
increased blood urea
on 13th August 2023
decreased Hb, increased total count,
increased neutrophils
decreased lymphocytes
ANTI HCV antibodies:
APTT:
BT & CT
Blood grouping:
Blood lactate:
Blood sugar random:
HBsAg
HIV:
LFT:
Increased total BR, direct BR, AKP
too decreased total proteins, albumin
PT:
RFT:
urinary urea increased, increased creatinine, hypocalcemia
BLOOD UREA:
increased
ECG:
15th aug 2023
HEMOGRAM: decreased Hb, increased total count,
increased neutrophils
decreased lymphocytes
ECG: 15-8-23
S.Creatinine
16-8-23
HEMOGRAM: decreased Hb, increased total count,
increased neutrophils
decreased lymphocytes
RFT: Increased urea, hypocalcemia, hypokalemia,
2D ECHO DOPPLER:
SINUS ARRHYTHMIA
Moderate to severe MR+, eccentric MR+, Moderate TR+ with PAH,
Grade I diastolic dysfunction, NO PE.
Calcified AV, thickened AV, Dilated L.A/ R.A
IVC size(1.68 cm) dilated collapsing
CHEST X RAY:
lower lobe consolidations
HEMOGRAM: decreased Hb, increased total count,
increased neutrophils
decreased lymphocytes
RFT:
USG:
renal cortical cyst
mild pleural effusion (l>r)
B/L grade 1 RFD changes
S. magnesium
Urinary chloride
Urinary potassium
Urine sodium
Pus culture :- coagulase negative staphylococci
USG chest: Free fluid in rt pleural space and left (r>l)
blood culture:
urine culture:
17-8-23
Hemogram: decreased Hb, Increased total count, decreased lymphocytes,
decreased PCV, decreased RBC count
LFT: increased total BR, Direct BR, AKP increased (4x),
too decreased total proteins and albumin
S. electrolytes
Peripheral smear:
Reticulocyte count:
18-8-23
Hemogram: Decreased Hb, Increased total count,
decreased lymphocytes, absent eosinophils,
decreased PCV, low RBC count
S. electrolytes:
19-8-23
Hemogram:
decreased Hb , increased total count,
decreased lymphocytes, low PCV, low RBC count
RFT: decreased uric acid, hypocalcemia
X ray
PROVISIONAL DIAGNOSIS:
SEPTIC SHOCK 2° LOWER LIMB CELLULITIS
WITH HYPOKALEMIA (under evaluation )
ć AKI (RESOLVING)
Acute on chronic cellulitis??
INFECTIVE ENDOCARDITIS???? (no vegetations found in echo )
With BILATERAL LOWER LOBES CONSOLIDATION
RIGHT MODERATE PLEURAL EFFUSION WITH COLLAPSE AND CONSOLIDATION
LEFT MILD PLEURAL EFFUSION
H/O PULMONARY KOCH'S 8 YRS BACK
H/O RHD??
MANAGEMENT:
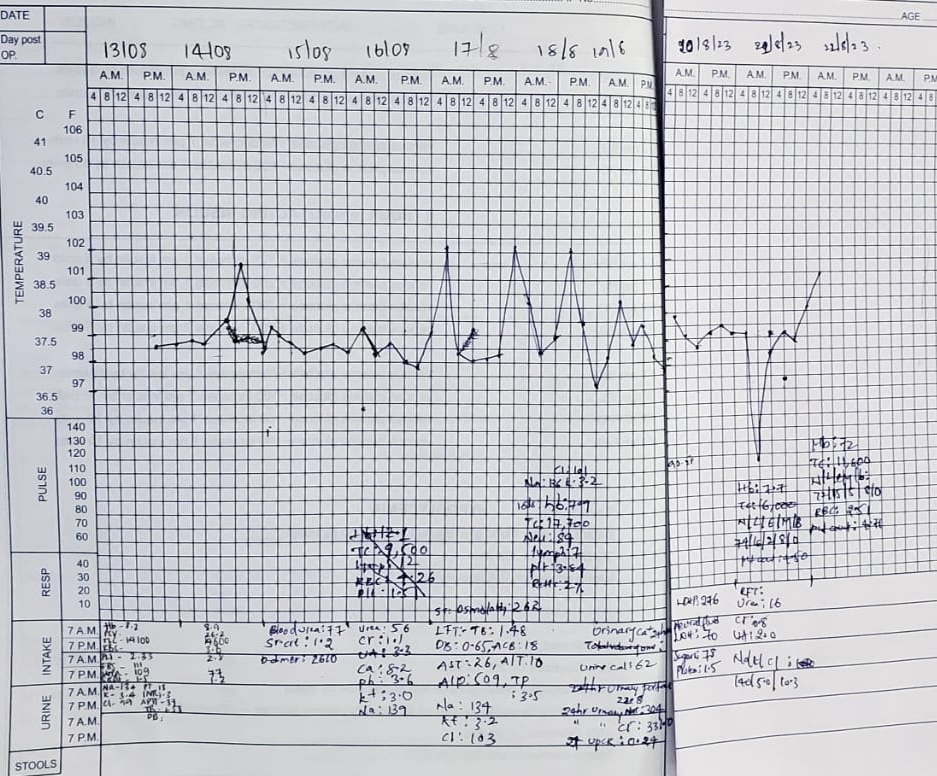
Day 1 : (13-8)
Inj peptaz
Inj pantop
Inj zofer
Inj tramadol
IVF 20RL, 20NS, 20.5%D
Lower limb end evaluation
Mgso4 + glycerine dressing
T/BP/PR hourly monitoring
GRBS 4th hrly
I/O charting
Inform surgery sos
Day 2 (14-8):
Soft diet
Inj noradrenaline
IVF 30RL , 10NS , 100 NS
Inj peptaz
Inj pantop
Inj zofer
Inj tramadol
Lower limb end evaluation
Mgso4 + glycerine dressing
T/BP/PR hourly monitoring
GRBS 4th hrly
I/O charting
Day 3 (15-8):
Soft diet
IVF 10 RL 10 NS @75ml/hr
Inj piptaz
Inj norad
Inj pan 40
Inj tramadol
Inj Neomol 1gm/IV (if temp >101F)
Inj zofer
Left LL end elevation
Mgso4 dressing
BP,PR,RR,SpO2 monitoring hourly
GRBS 4th hrly
Strict I/O charting
Day 4(16-8):
Soft diet
IVF 10 RL 10 NS @75ml/hr
Inj piptaz
Inj norad
Inj pan 40
Inj tramadol
Inj Neomol 1gm/IV (if temp >101F)
T.PCM
Inj zofer
Left LL end elevation
Mgso4 dressing
BP,PR,RR,SpO2 monitoring 4th hourly
GRBS 4th hrly
Strict I/O charting
Syp Cremaffin
Syp potklor 15ml
Day 5(17-8):
IVF 30NS @50ml/hr
Inj piptaz
Inj norad
Inj pan 40
Inj Neomol 1gm/IV (if temp >101F)
T.PCM
Left LL end elevation
Mgso4 dressing
BP,PR,RR,SpO2 monitoring 2 hourly
GRBS 4th hrly
Strict I/O charting
Syp potklor 15ml
2 egg whites daily
Protein powder 2 cups in 1 glass of milk
Inj Metrogyl 500mg
Day 6(18-8):
IVF 30NS 50ml/hr
Inj piptaz
Inj norad
Inj pan 40
Inj Neomol 1gm/IV (if temp >101F)
T.PCM
Inj zofer
Left LL end elevation
Mgso4 dressing
BP,PR,RR,SpO2 monitoring hourly
GRBS 4th hrly
Strict I/O charting
Syp potklor
2 egg whites daily
Protein powder 2 cups in glass of milk or water
T orofer xt
Day 7(19-8):
IVF NS @50ml/hr
Inj peptaz
Inj metrogyl
Inj neomol
Inj norad
T PCM
Syp potklor
2 egg whites daily
Protein powder 2 cups in glass of milk or water
T orofer xt
GRBS Monitoring
BP,PR,RR monitoring hrly
Strict I/O charting
Day 8(20-8)
IVF NS@50ml/hr
INJ PIPTAZ
INJ METROGYL
Inj Neomol
Inj Norad
T. PCM
T. orofer
Protein powder 2 spoons in 1 glass of water or milk
2 egg whites daily
GRBS monitoring
BP, PR, RR hourly
Temp monitoring 4th hrly
Strict I/O Charting
Day 9 (21-8)
IVF NS@50ml/hr
INJ PIPTAZ
INJ METROGYL
Inj Neomol
Inj Norad
T. PCM
T. orofer
Protein powder 2 spoons in 1 glass of water or milk
2 egg whites daily
GRBS monitoring
BP, PR, RR 4th hourly
Temp monitoring 4th hrly
Strict I/O Charting
Day 10 (22-8)
Lost this patient while treatment is going on. 🙏🏻
.jpeg)

















.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)
.jpeg)

.jpeg)

.jpeg)

.jpeg)
.jpeg)
.jpeg)
.jpeg)















































.png)
.png)


No comments:
Post a Comment